

Post-traumatic stress disorder (PTSD) is a disorder that develops in some people who have experienced a shocking, scary, or dangerous event.
It is natural to feel afraid during and after a traumatic situation. Fear triggers many split-second changes in the body to help defend against danger or to avoid it. This “fight-or-flight” response is a typical reaction meant to protect a person from harm. Nearly everyone will experience a range of reactions after trauma, yet most people recover from initial symptoms naturally. Those who continue to experience problems may be diagnosed with PTSD. People who have PTSD may feel stressed or frightened, even when they are not in danger.
signs and symptoms
While most but not all traumatized people experience short term symptoms, the majority do not develop ongoing (chronic) PTSD. Not everyone with PTSD has been through a dangerous event. Some experiences, like the sudden, unexpected death of a loved one, can also cause PTSD. Symptoms usually begin early, within 3 months of the traumatic incident, but sometimes they begin years afterward. Symptoms must last more than a month and be severe enough to interfere with relationships or work to be considered PTSD. The course of the illness varies. Some people recover within 6 months, while others have symptoms that last much longer. In some people, the condition becomes chronic.
A trauma-informed practitioner who has experience helping people with mental illnesses, such as a psychiatrist or psychologist, can diagnose PTSD. To be diagnosed, an adult must have all of the following for at least 1 month:
- At least one re-experiencing symptom
- At least one avoidance symptom
- At least two arousal and reactivity symptoms
- At least two cognition and mood symptoms
Re-experiencing symptoms include
- Flashbacks—reliving the trauma over and over, including physical symptoms like a racing heart or sweating
- Bad dreams
- Frightening thoughts
Re-experiencing symptoms may cause problems in a person’s everyday routine. The symptoms can start from the person’s own thoughts and feelings. Words, objects, or situations that are reminders of the event can also trigger re-experiencing symptoms.
Avoidance symptoms include:
- Staying away from places, events, or objects that are reminders of the traumatic experience
- Avoiding thoughts or feelings related to the traumatic event
Things that remind a person of the traumatic event can trigger avoidance symptoms. These symptoms may cause a person to change his or her personal routine. For example, after a bad car accident, a person who usually drives may avoid driving or riding in a car.
Arousal and reactivity symptoms include:
- Being easily startled
- Feeling tense or “on edge”
- Having difficulty sleeping
- Having angry outbursts
Arousal symptoms are usually constant, instead of being triggered by things that remind one of the traumatic events. These symptoms can make the person feel stressed and angry. They may make it hard to do daily tasks, such as sleeping, eating, or concentrating.
Cognition and mood symptoms include:
- Trouble remembering key features of the traumatic event
- Negative thoughts about oneself or the world
- Distorted feelings like guilt or blame
- Loss of interest in enjoyable activities
Cognition and mood symptoms can begin or worsen after the traumatic event, but are not due to injury or substance use. These symptoms can make the person feel alienated or detached from friends or family members.
It is natural to have some of these symptoms for a few weeks after a dangerous event. When the symptoms last more than a month, seriously affect one’s ability to function, and are not due to substance use, medical illness, or anything except the event itself, they might be PTSD. Some people with PTSD don’t show any symptoms for weeks or months. PTSD is often accompanied by depression, substance abuse, or one or more of the other anxiety disorders.
Children and teens can have extreme reactions to trauma, but some of their symptoms may not be the same as adults. Symptoms sometimes seen in very young children (less than 6 years old), these symptoms can include:
- Wetting the bed after having learned to use the toilet
- Forgetting how to or being unable to talk
- Acting out the scary event during playtime
- Being unusually clingy with a parent or other adult
Older children and teens are more likely to show symptoms similar to those seen in adults. They may also develop disruptive, disrespectful, or destructive behaviors. Older children and teens may feel guilty for not preventing injury or deaths. They may also have thoughts of revenge.
risk factors
Anyone can develop PTSD at any age. This includes war veterans, children, and people who have been through a physical or sexual assault, abuse, accident, disaster, or other serious events. According to the National Center for PTSD, about 7 or 8 out of every 100 people will experience PTSD at some point in their lives. Women are more likely to develop PTSD than men, and genes may make some people more likely to develop PTSD than others.
Not everyone with PTSD has been through a dangerous event. Some people develop PTSD after a friend or family member experiences danger or harm. The sudden, unexpected death of a loved one can also lead to PTSD.
why do some people develop PTSD and others don’t?
It is important to remember that not everyone who lives through a dangerous event develops PTSD. In fact, most people will not develop the disorder. Many factors play a part in whether a person will develop PTSD. Some examples are listed below. Risk factors make a person more likely to develop PTSD. Other factors, called resilience factors, can help reduce the risk of the disorder.
Some factors that increase risk for PTSD include:
- Living through dangerous events and traumas
- Getting hurt
- Seeing another person hurt, or seeing a dead body
- Childhood trauma
- Feeling horror, helplessness, or extreme fear
- Having little or no social support after the event
- Dealing with extra stress after the event, such as loss of a loved one, pain and injury, or loss of a job or home
- Having a history of mental illness or substance abuse
Some factors that may promote recovery after trauma include:
- Seeking out support from other people, such as friends and family
- Finding a support group after a traumatic event
- Learning to feel good about one’s own actions in the face of danger
- Having a positive coping strategy, or a way of getting through the bad event and learning from it
- Being able to act and respond effectively despite feeling fear
Researchers are studying the importance of these and other risk and resilience factors, including genetics and neurobiology. With more research, someday it may be possible to predict who is likely to develop PTSD and to prevent it.
treatments and therapies
Everyone is different, and PTSD affects people differently, so a treatment that works for one person may not work for another. It is important for anyone with PTSD to be treated by a mental health provider who is experienced with PTSD. Some people with PTSD may need to try different treatments to find what works for their symptoms.
If someone with PTSD is going through an ongoing trauma, such as being in an abusive relationship, both of the problems need to be addressed. Other ongoing problems can include panic disorder, depression, substance abuse, and feeling suicidal.
medications -the most studied type of medication for treating PTSD are antidepressants, which may help control PTSD symptoms such as sadness, worry, anger, and feeling numb inside. Other medications may be helpful for treating specific PTSD symptoms, such as sleep problems and nightmares.
psychotherapy – psychotherapy (sometimes called “talk therapy”) involves talking with a mental health professional to treat a mental illness. Psychotherapy can occur one-on-one or in a group. Talk therapy treatment for PTSD usually lasts 6 to 12 weeks, but it can last longer. Research shows that support from family and friends can be an important part of recovery.
Many types of psychotherapy can help people with PTSD. Some types target the symptoms of PTSD directly. Other therapies focus on social, family, or job-related problems. The therapist may combine different therapies depending on each person’s needs.
Effective psychotherapies tend to emphasize a few key components, including education about symptoms, teaching skills to help identify the triggers of symptoms, and skills to manage the symptoms. One helpful form of therapy is called cognitive behavioral therapy, or CBT. CBT can include:
- Exposure therapy. This helps people face and control their fear. It gradually exposes them to the trauma they experienced in a safe way. It uses imagining, writing, or visiting the place where the event happened. The therapist uses these tools to help people with PTSD cope with their feelings.
- Cognitive restructuring. This helps people make sense of the bad memories. Sometimes people remember the event differently than how it happened. They may feel guilt or shame about something that is not their fault. The therapist helps people with PTSD look at what happened in a realistic way.
Talk therapies teach people helpful ways to react to the frightening events that trigger their PTSD symptoms. Based on this general goal, different types of therapy may:
- Teach about trauma and its effects
- Use relaxation and anger-control skills
- Provide tips for better sleep, diet, and exercise habits
- Help people identify and deal with guilt, shame, and other feelings about the event
- Focus on changing how people react to their PTSD symptoms. For example, therapy helps people face reminders of the trauma.
neurofeedback
Neurofeedback is one of the new promising, evidence-based therapies that can help address the deeper, underlying biological changes that result from trauma and PTSD. Trauma is stored in deeper parts of the brain and nervous system as whole-body experiences, not just linear narratives. This means that patients don’t just remember what happened as a coherent story – they also remember how they felt and how their bodies reacted. They remember how scared they were, as well as their racing heart and difficulty breathing.
Talk therapy often cannot address these emotional and physical memories of trauma that have become ingrained in the body’s biology. Additionally, one study found that about 40% of patients in the community with PTSD drop out from CBT (cognitive behavioral therapy), the most recommended type of talk therapy for trauma. Patients need a more comprehensive type of treatment with better outcomes.
Trauma takes away a person’s sense of safety and stability at a deep, core level and activates the amygdala. The amygdala is part of the limbic system, a deeper, more primitive part of the brain that primarily responds to basic signals about fear and safety. Here, memory is stored as a lived experience with feelings and physical sensations that may not be connected in a logical story.
Talk therapy works at the prefrontal cortex where we plan, learn, and organize, but it does not communicate as well with the limbic system. In other words, talk therapy can appeal to our sense of reasoning and language, but it doesn’t speak to the deeper parts of the brain that experience and store the memories of trauma.

“The Body Keeps the Score”*
During a traumatic event, the amygdala alerts the hypothalamus, a part of the brain that coordinates the body’s stress response by producing hormones like cortisol. In addition, the autonomic nervous system – which controls our involuntary body functions – goes into fight-or-flight mode. This means having a faster heart rate, breathing more shallowly, sweating, and not being able to think clearly.
In this way, trauma can change the body’s biology. Even after the trigger is gone, the amygdala can hold onto the physical memory of trauma, and our bodies can get stuck in this fight-or-flight mode, leaving us with higher levels of cortisol and symptoms of hyperarousal.
While we can ask someone to calm down and think more rationally, that may not change their whole-body response to trauma. We need trauma treatments that can heal the brain and body’s biology.
*“Traditionally we’ve tried to heal PTSD through talking and making meaning of the event, but treatment methods that help calm arousal systems in the deeper regions of the brain have been helpful in calming PTSD more than those that try to do so through talking and reasoning.”
— Dr Bessel Van der Kolk
Neurofeedback is a non-invasive, evidence-based treatment that can encourage healthier brain function through brainwave training. Our brain cells communicate through electrical impulses, also known as brainwaves. Normal brainwave patterns can be disrupted by trauma, resulting in patients getting stuck in unhealthy patterns of biological activity and behavior. Neurofeedback can help the brain become more flexible and develop healthier patterns and responses, a process known as neuroplasticity.
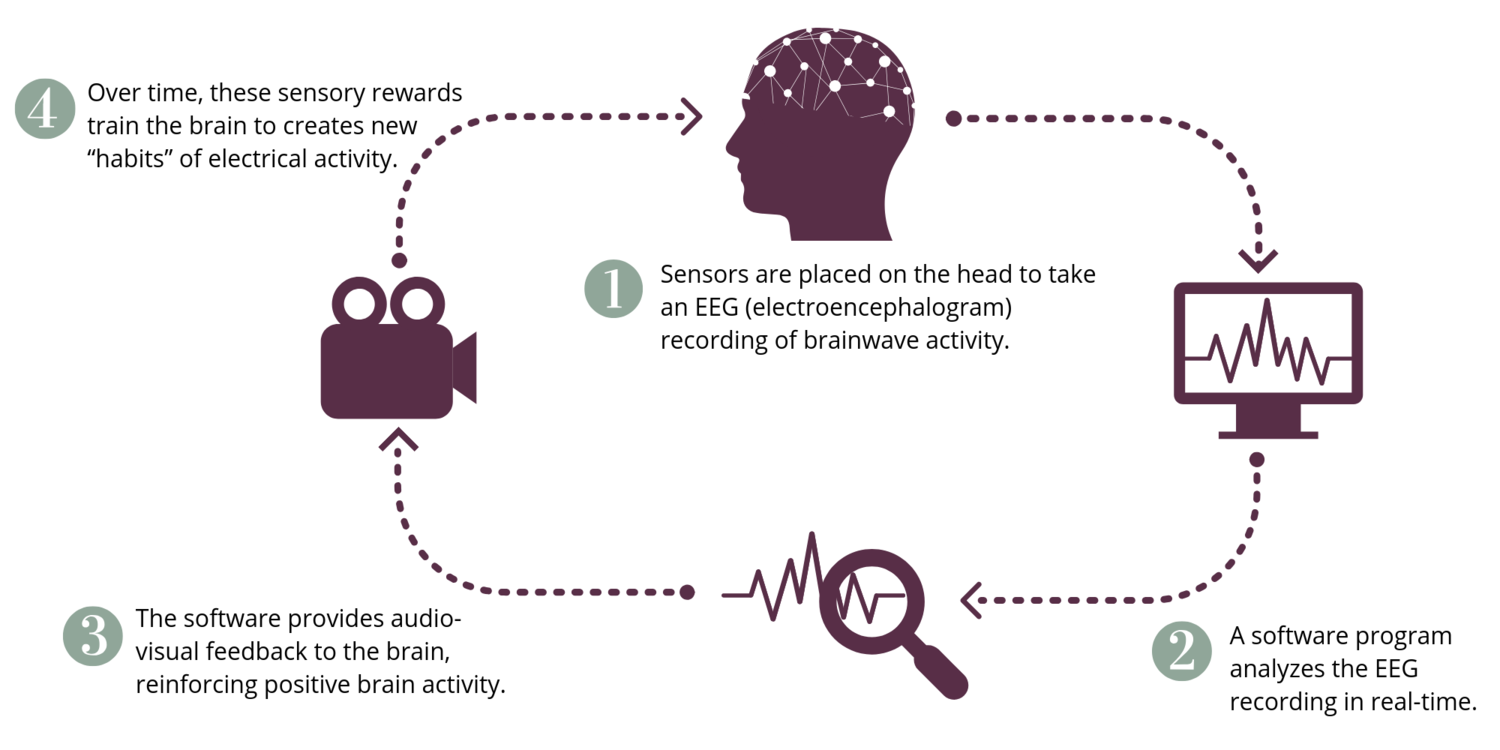
When a patient’s brainwave activity moves into a healthier state, the brain is rewarded with pleasant video and audio. Our brains, just like animals, are constantly seeking rewards. During a single neurofeedback session, the brain is given multiple opportunities to self-correct and be rewarded.
Since neurofeedback doesn’t require patients to talk about past events, they can relax and let their brains do the work for them. However, it is important that patients have a licensed mental health provider to speak to if associations, feelings, or memories come up during or after the session.
The goal of trauma-focused neurofeedback is to help shift people from a hyper-aroused state to a calmer one so that they can experience a sense of safety and react more appropriately to everyday events. There have been many studies showing that neurofeedback can help with symptoms of PTSD. Some have even shown that neurofeedback can change brain function of PTSD patients on imaging or fMRI.
Furthermore, the level of symptom improvement in most of these studies has been significant. In fact, the effect size with neurofeedback in many studies has been greater than any medication used for PTSD.
Credits:
Main article curated from National Institute for Mental Health https://www.nimh.nih.gov/ post traumatic stress disorder
Section on neurofeedback curated from Saruchi Chandra MD, Integrative Psychiatry & Medicine https://www.chandramd.com/blog/neurofeedback-trauma-ptsd
“The Body Keeps the Score: Mind, Brain and Body in the Transformation of Trauma” – Bessel Van der Kolk
