

The vagus nerves are the nerves of life. They keep us alive by their innervation of the internal organs of the body and their interactions with the brain, spinal cord, cranial nerves, upper cervical spinal nerves, and sympathetic nervous system. Sensory functions of the vagus nerve are critical for conscious perception and for monitoring visceral functions in the cardiopulmonary and gastrointestinal systems. As such the vagus nerve has a critical role in the maintenance of bodily homeostasis (balance) in diverse functions relating to digestion, satiety, respiration, blood pressure, and heart rate control. Its profound role is illustrated by abnormalities in it that can lead to far-reaching consequences including gastroesophageal reflux disease, heart failure, failure of respiratory control, gastroparesis, vasovagal syncope, and chronic pain.
The interference of vagus nerve signals and function leads to cervicovagopathy, a condition caused by cervical instability and a breakdown of the cervical curve, called cervical dysstructure. The dysautonomia (nerve dysfunction) produced leads to overall sympathetic dominance (or parasympathetic deficiency. A state of constant stress or “fight or flight” mode.)
The vagus nerve seems to extend everywhere; consider: the supradiaphragmatic vagus nerve innervates the skin of the external acoustic meatus (auricular branch) and the dura of the posterior cranial fossa (meningeal branch), larynx, pharynx, and upper esophagus (pharyngeal branches), aortic arch (cervical cardiac branches), trachea and esophagus (recurrent laryngeal), lungs and heart.
The right vagus nerve (more so than the left) innervates the SA node and the AV node of the heart. (This is why vagus nerve stimulators are placed on the left side). The subdiaphragmatic vagus nerve innervates the liver, pylorus, antrum, pancreas, intestine, and stomach. Efferent vagus branches reach the uterus, adrenal gland, and gallbladder. Vagus nerve fibers innervate the thymus and travel to abdominal adipose tissue. The vagus nerve has many branches that interacts with the enteric nervous system and provides central coordination of everything related to the digestive tract, including sensation, absorption, motility and even sphincter control.
Below we will discuss how these symptoms and conditions can be monitored by heart rate variability. As the condition of cervicovagopathy progresses, almost any human illness throughout the body can occur. Treatment is directed to improve the structural integrity of the cervical spine and the pathophysiology it causes including cervicovagopathy and increased intracranial pressure. Treatment modalities can include dynamic (chiropractic) orthoneurological adjustments for the vertebral subluxations (malrotations), curve correction to restore lordosis and Prolotherapy to repair injured ligaments. The diagnostic tests used to discover the ligamentous cervical instability and resultant pathophysiology can also be used to monitor to progress during treatment.
The vagus nerve plays a key role in regulating many of our body’s functions. Its name best describes its physical characteristic, Vagus is Latin for “fugitive,” or “wanderer.” It is the longest and most widely extended of the nerves of the body.
The vagus nerve is also noted as being the tenth cranial nerve (designated as CN X). The vagus nerve is actually a set of two nerves, a vagus nerve right side of the neck and a vagus nerve left side of the neck.
The vagus nerve is a 2-way messenger network, passing messages and signals between the organs and brain to maintain heart rate, blood pressure, circulation, breathing, internal organ distension (for example the moving of food through the digestive system), secretions, and inflammation. As we will see below the vagus nerve helps us talk, swallow, focus vision, hear, and understand. The vagus nerve also sends out messages as part of the parasympathetic nervous system that “calms down” the body after physical exertion or in response to stress in a “fight or flight” situation.

article summary
In this article, I will briefly discuss an incredible number of symptoms and conditions in the human body that can be caused by disruption of and interference of the vagus nerve signals. I will also provide more detailed information on each disorder and symptom through links to companion articles on this website.
I will also focus on one mechanism by which vagus nerve dysfunction can be altered. That is through the mechanism of cervicovagopathy. Cervico – a structural problem in the neck that is causing “vago” vagus nerve “pathy” or disease or illness. See my article Cervical Myelopathy – Cervical Degenerative Disc Disease – Cervicovagopathy. Cervicovagopathy is then the neck’s altered or broken structure causing compression or disease on the vagus nerve and then on to produce a myriad of symptoms, as either structural and/or systemic disease causes.
very complex medical history
We have seen many patients who have a very complex medical history. In some cases, they would describe a dozen or more disorders. The patient will tell us that if they had gastrointestinal distress, the gastrointestinal specialist treated them. If they had cardiovascular-type symptoms, a slow or racing heartbeat for example, or spells of passing out, they were referred to the heart specialist. Problems with earing or tinnitus were sent to the otologist, problems with vision would send them to the ophthalmologist, skin problems were seen by the dermatologist, urinary problems by the urologists, etc. Sometimes a psychiatrist would often be referred.
Sometimes the psychiatrist would be the last referral because the patient has started a process of denial. Not because they denied they had all these things wrong with them, but they started to deny that treatments they were getting were in fact getting anywhere. These people would summarize the above experiences as years of each disorder being treated as its own cause and effect, in isolation, with symptomatic treatment. Rarely were all these problems that these people addressed through a singular cause.
Intuitively patients knew that “something had to be at the bottom of all this.” Somehow dizziness, digestive problems, ringing in the ears, blurry vision, itching, poor body temperature control, brain fog, choking sensations, depression, anxiety, inability to focus and other symptoms had to somehow all be related.
sensory functions of the vagus nerve
In the neck, the vagus nerve connects to the inferior, middle, and superior cervical sympathetic ganglion (SCSG), as well as the upper cervical nerves and many of the cranial nerves and descends all the way down to the celiac plexus, the nerves that innervate the abdomen.
The inferior cervical sympathetic ganglion is a nerve complex located between the C7 and the top rib. Messages between the vagus nerve and inferior cervical sympathetic ganglion influence blood flow between the heart, brain, and neck. Altered messages between the vagus nerve and the inferior cervical sympathetic ganglion can impact the function of the subclavian arteries supply blood to the thorax, head, neck, shoulder, and arms.
Fainting, loss of blood flow to the brain: Subclavian arteries branch off into the vertebral artery which supplies blood to the back of the brain through the basilar, posterior cerebral, and cerebellar arteries. Dysfunction can cause blackouts, fainting, and vascular problems.
Thyroid :The vagus nerve connects to the external laryngeal nerves which act upon the inferior thyroid artery.
Cardiovascular risks: The thyroid receives its nerve supply mainly from the middle cervical ganglion but also is innervated by the superior and inferior cervical ganglions.
A study published in the North American Journal of Medical Sciences (1) investigated the link between sympathovagal imbalance (Sympathovagal imbalance is the disruption and dysfunction in which the sympathetic and vagal components of the autonomic nervous system run either too high or too low. In other words, too much “flight-fight” or too little and problems with energy, fatigue, and digestion among many symptoms) to cardiovascular risks and the plausible mechanisms of cardiovascular risks in hypothyroidism. What the researchers suggested was sympathovagal imbalance could be implicated in:
- Increased diastolic pressure (the bottom number of a blood pressure reading).
- Decreased HRV (Heart rate variable) and increased low-frequency to the high-frequency ratio (LF-HF) of HRV.
- Dyslipidemia (Cholesterol problems).
- Increased high-sensitive C-Reactive Protein (inflammation)
All these symptoms were observed in hypothyroid patients and all these parameters had a significant correlation with the heart rate variability. Sympathovagal imbalance due to sympathetic activation and vagal withdrawal occurs in hypothyroidism.
Blood pressure: A February 2018 study in the journal Biomed Central Research (2) notes examined the effect of propranolol (blood pressure medication) on heart rate variability (HRV) in hyperthyroidism before antithyroid treatment. This was a before and after study, on ten patients presenting overt hyperthyroidism who had no previous treatment.
HRV parameters including sympathovagal balance estimate by low-frequency to the high-frequency ratio (LF-HF) ratio remained unchanged. Although a significant reduction in heart excitability, propanolol failed to restore a good sympathovagal balance in hyperthyroidism.
Neck pain and cervical spine surgery and injury. Many of the people that we see in our practice have been on a long medical journey as described above. They are at our center because a connection between neck pain and neck injury has been made. There is a suspicion that a structural cause, that is cervical instability, or floating vertebrae or neck bones, is the cause of the compression on the vagus nerve and a condition of Cervicovagopathy. This would be seen in patients with a medical history of post-concussion syndrome, Whiplash Associated Disorder, cervical spine fusion or cervical spine laminectomy, and hypermobility Ehlers-Danlos Syndrome.
How does one come to a condition of Cervicovagopathy or wandering floating neck bones? This condition is caused by weakened, loose, and damaged cervical spine ligaments. Ligaments are the soft-tissue structure that holds the vertebrae in place. When these ligaments no longer hold the vertebrae in place the structure of the neck falters and the natural curve of the cervical spine is lost. This condition is described in the image below.
The progressive nature of cervical instability that leads to a breakdown of the cervical curve resulting in destructive forces (compression, grinding, and impingement of blood vessels and nerves) being placed on vital neurovascular structures including the cervical spinal cord and vagus nerves. This all occurs because of damage to the cervical spine ligaments that hold the bones in proper alignment.
- NORMAL posture.
- MILD cervical spine instability, the head is moving forwards causing a mild stretch of the nerves and blood vessels. When blood vessels are stretched, the vessels narrow.
- MILITARY Neck: This condition is called a military neck because the neck is standing up straight. This is not a good thing. The spine acts as a shock absorber and is built like a spring with a curve to it.
- KYPHOTIC. The cervical spine instability has become so severe, that the curve of the neck has reversed itself and is now backward.

Treatment for loss of natural neck curve structure is directed to improve the structural integrity of the cervical spine and the symptoms and conditions it causes, including cervicovagopathy and increased intracranial pressure. Treatment modalities can include dynamic (chiropractic) orthoneurological adjustments for the vertebral subluxations (malrotations), curve correction to restore lordosis, and Prolotherapy to repair injured ligaments. The diagnostic tests used to discover cervical instability and resultant pathophysiology can also be used to monitor progress during treatment. These treatment options are discussed below. Please also see our article on treatments for Atlas displacement c1 forward misalignment.
causes of vagal or parasympathetic dysfunction
The etiology of the cause of vagal or parasympathetic dysfunction has many chemical and emotional etiologies, including diabetes, heavy metals, medications, and emotional or financial stress, but a cause that is overlooked is structural injury. As the list of symptoms and diseases, including chronic pain, depression, tinnitus, migraine headache, seizures, heart failure, Alzheimer’s dementia, and systemic inflammation continues to grow, it is prudent that clinicians and the patients they treat understand the vagus nerve anatomy, injury, and the pathophysiology it causes.
External laryngeal nerves – voice, breathing, swallowing problems. The plexus (bundle of nerves and blood vessels) on the inferior thyroid artery talks with the recurrent and external laryngeal nerves, with the superior cardiac nerve, and with the plexus on the common carotid artery. Laryngeal nerve dysfunction can cause loss of voice, hoarseness, swallowing difficulties and a sense of breathing obstruction.
The phrenic nerve – breathing, swallowing, and hiccups. The phrenic nerve sends messages through the thorax to assist in regulating breathing, controlling the cough reflex, and the hiccup reflex.
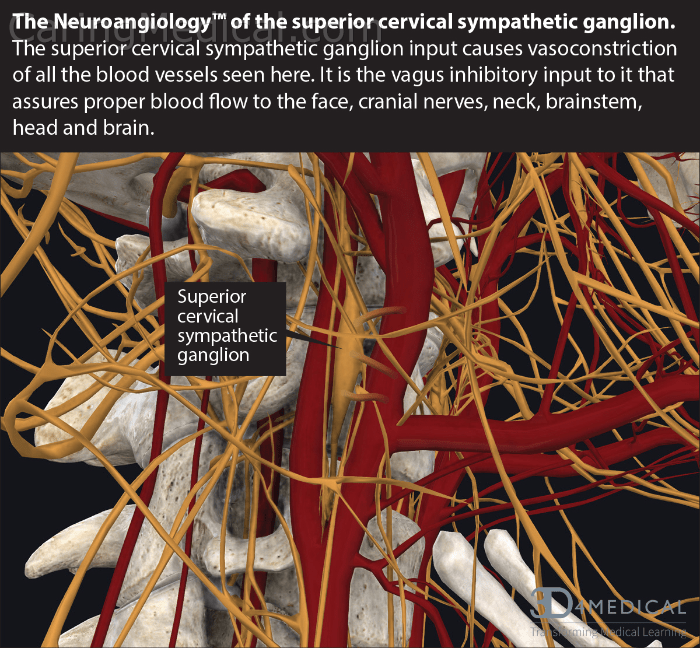
The image below shows the superior cervical sympathetic ganglion in its native habitat. Surrounded by blood vessels (internal carotid artery and internal jugular vein) and nerve networks and near the C2 vertebrae. When the vertebrae wander out of position, it takes these veins, arteries, nerves, and nerve bundles with it, causing compression and stretching of these vital structures. In the context of this article, this compression and stretching can not only cause pain but disrupt nerve signals causing neurologic-like symptoms and conditions already outlined in this article.
The vagus nerve has five main components contained within the nerve, which make up the five fascicles or nerve bundles seen in vagus nerve cross sections. These are branchial motor, visceral sensory, visceral motor, and special and general sensory fibers. (See Figure). These five vagus nerve components can be summarized:
- Special visceral afferent (SVA, motor) – these motors are special because they supply motor innervation to skeletal muscles of branchial arch origin which include all the muscles of the pharynx, larynx, and soft palate.
- General visceral efferent (GVE, motor) – contains the parasympathetic motor part of the nerve that innervates the smooth muscles of the trachea, bronchi, and gastrointestinal tract and regulates heart rhythm. When we talk about the vagal tone we are talking about this part of the vagus nerve primarily. It is the part that slows the heart rate and is responsible for sinus arrhythmia with breathing.
- General visceral afferent (GVA, sensory) – general sensory to the abdominal viscera including the trachea, larynx, and oesophagus digestive tract.
- Special visceral afferent (SVA, sensory) – taste sensation to the epiglottis and root of the tongue.
- General sensory afferent (GSA)– these fibers carry general sensation ( touch, pressure, pain, and temperature) from cutaneous structures and mucous membranes of the head, and general proprioception from somatic structures such as muscles, tendons, and joints of the head and neck. The trigeminal, facial, glossopharyngeal, and vagus nerves transmit GSA input to the spinal nucleus of the trigeminal nerve. One important innervation is to the skin of the external acoustic meatus, which is used for transcutaneous auricular vagus nerve stimulation.
cervicovagopathy
The role of vagus nerve function in health and disease cannot be overemphasized. The hallmarks of dysautonomia (conditions and symptoms caused by problems with the autonomic nervous system (ANS))—parasympathetic dysfunction causing sympathetic dominance, or what is termed “sympathovagal imbalance”—are paramount to understanding the pathophysiology of most medical conditions. The role of sympathovagal imbalance, discussed briefly above will continue to be a dominating theme within this article.
Cervicovagopathy is defined as degeneration of the vagus nerve and/or interruption of vagal nerve impulses from the effects of damaged ligaments causing cervical instability, with or without significant cervical dysstructure or advanced cervical structural problems, leading to harmful effects on the body. Cervicovagopathy is one of the most devastating effects of cervical instability, upper cervical instability, and cervical dysstructure.
In the image below we see x-ray evidence of cervical spine misalignment, cervical dysstructure, and cervical spine instability. In the top panel, we see a misalignment of the C2. In the center panel, we see cervical dysstructure and a comparison of where a normal cervical curve should be and a significant curve structural problem causing the vertebrae to be displaced by 2 – 3 inches. The vagus nerve is associated with C1. In the lower panel, we see how far off-set the vertebrae are from each other and from C2-C6.

Now let’s re-examine the discussion we had above about Heart Rate Variability
Homeostasis of the human body is under the control of the autonomic nervous system (ANS); while the sympathetic nerve system (SNS) allows us to handle stress, the parasympathetic nervous system (PNS) allows us to live. As the vagus nerve is the primary sensory input and effector for the parasympathetic nervous system, its compromise has many long-ranging detrimental effects on human homeostasis and health.
When the autonomic nervous system (ANS) balance becomes sympathetic dominant, a rise in the LF/HF ratio is seen on Heart Rate Variable parameters. This rise in LF/HF ratio is frequently found in many chronic diseases, which brings up the hypothesis that the chronic symptoms these conditions produce may have as their etiology the breakdown of the cervical curve, affecting the precise balance between sympathetic and parasympathetic function—a condition known as dysautonomia. If this is true, then treatment should be directed at improving the cervical structure and stability to restore body vagal tone.
This blog is Part I of an edited article originally published by Caring Medical Regenerative Medicine Center. Parts II and III will look at understanding treatment for Cervicovagopathy and treatment modalities.
About the author: Ross Hauser MD. Medical Director, Caring Medical Regenerative Medicine Center, Fort Myers, Florida, USA
Board Certified Physiatrist (or Physical Medicine and Rehabilitation Specialist): completed residency training in Physical Medicine and Rehabilitation at Loyola Medical Center in Chicago; MD University of Illinois, Chicago; and Bachelor of Science undergraduate degree from the University of Illinois, Urbana-Champaign.
References:
1 Syamsunder AN, Pal GK, Pal P, Kamalanathan CS, Parija SC, Nanda N. Association of sympathovagal imbalance with cardiovascular risks in overt hypothyroidism. North American Journal of Medical Sciences. 2013 Sep;5(9):554. [Google Scholar]
2 Tankeu AT, Azabji-Kenfack M, Nganou CN, Ngassam E, Kuate-Mfeukeu L, Mba C, Dehayem MY, Mbanya JC, Sobngwi E. Effect of propranolol on heart rate variability in hyperthyroidism. BMC Research Notes. 2018 Dec;11(1):1-4. [Google Scholar]
3 De Couck M, Mravec B, Gidron Y. You may need the vagus nerve to understand pathophysiology and to treat diseases. Clinical science. 2012 Apr 1;122(7):323-8. [Google Scholar]
4. Mol MB, Strous MT, van Osch FH, Vogelaar FJ, Barten DG, Farchi M, Foudraine NA, Gidron Y. Heart-rate-variability (HRV), predicts outcomes in COVID-19. PLoS One. 2021 Oct 28;16(10):e0258841. [Google Scholar].
5 Diener HC, Gaul C, Holle-Lee D, Jürgens TP, Kraya T, Kurth T, Nägel S, Neeb L, Straube A. Headache-an Update 2018. Laryngo-Rhino-Otologie. 2019 Mar 7;98(3):192-217. [Google Scholar]
6 Guclu B, Sindou M, Meyronet D, Streichenberger N, Simon E, Mertens P. Cranial nerve vascular compression syndromes of the trigeminal, facial and vago-glossopharyngeal nerves: comparative anatomical study of the central myelin portion and transitional zone; correlations with incidences of corresponding hyperactive dysfunctional syndromes. Acta neurochirurgica. 2011 Dec;153(12):2365-75. [Google Scholar]
7 Taher F, Bokums K, Aichmair A, Hughes AP. C1–C2 instability with severe occipital headache in the setting of vertebral artery facet complex erosion. European Spine Journal. 2014 May;23(2):145-9. [Google Scholar]
8 Sleigh JN, Rossor AM, Fellows AD, Tosolini AP, Schiavo G. Axonal transport and neurological disease. Nature Reviews Neurology. 2019 Dec;15(12):691-703. [Google Scholar]
9 Yolas C, Kanat A, Aydin MD. Unraveling of the effect of nodose ganglion degeneration on the coronary artery vasospasm after subarachnoid hemorrhage: an experimental study. World Neurosurg. 2016 Feb;86:79-87 [Google Scholar]
10 Atalay C, Gundogdu B, Aydin MD. Vagal ischemia induced lung immune component infarct following subarachnoid hemorrhage: an experimental study. Turk Neurosurg. 2017 Jan 1;27(4):509-15. [Google Scholar]
11 Soyalp C, Kocak MN, Ahiskalioglu A, Aksoy M, Atalay C, Aydin MD, Cakir M, Calikoglu C, Ozmen S. New determinants for casual peripheral mechanism of neurogenic lung edema in subarachnoid hemorrhage due to ischemic degeneration of vagal nerve, kidney and lung circuitry. Experimental study. Acta Cirúrgica Brasileira. 2019 Mar 18;34. [Google Scholar]
12 Shahrestani J, Das JM. Neuroanatomy, auerbach plexus. StatPearls [Internet]. 2021 Jun 4. [Google Scholar]
13 Cakir M, Ahiskalioglu A, Karadeniz E, Aydin MD, Malcok UA, Soyalp C, Calikoglu C, Sengul G, Sipal S, Yayik AM. A new described mechanisms of intestinal glandular atrophy induced by vagal nerve/Auerbach network degeneration following subarachnoid hemorrhage: The first experimental study. Journal of Clinical Neuroscience. 2019 Jan 1;59:305-9. [Google Scholar]
14 Karemaker JM. The multibranched nerve: vagal function beyond heart rate variability. Biological Psychology. 2022 Jun 7:108378. [Google Scholar]
15 Pigato G, Rosson S, Bresolin N, Toffanin T, Sambataro F, Olivo D, Perini G, Causin F, Denaro L, Landi A, D’Avella D. Vagus Nerve Stimulation in Treatment-Resistant Depression: A Case Series of Long-Term Follow-up. The Journal of ECT.:10-97. [Google Scholar]
